Frequently reported adverse events, drug related or not, were nausea (5.2%), diarrhea (2.3%), abdominal pain/discomfort (1.7%), headache (1.2%), restlessness (1.1%) and rash (1.1%).
Additional events which occurred in less than 1% of ciprofloxacin patients include the following:
Central nervous system: dizziness, lightheadedness, insomnia, nightmares, hallucinations, manic reaction, irritability, tremor, ataxia, convulsive seizures, lethargy, drowsiness, weakness, malaise, anorexia, phobia, depersonalization, depression, paresthesia.
Cardiovascular: palpitation, atrial flutter, ventricular ectopy, syncope, hypertension, angina pectoris, myocardial infarction, cardiopulmonary arrest, cerebral thrombosis.
Respiratory: dyspnea, epistaxis, laryngeal or pulmonary edema, hiccough, hemoptysis, bronchospasm, pulmonary embolism.
Gastrointestinal: painful oral mucosa, oral candidiasis, dysphagia, intestinal perforation, gastrointestinal bleeding. Cholestatic jaundice has been reported.
Skin/hypersensitivity: pruritus, urticaria, photosensitivity, flushing, fever, chills, angioedema, edema of the face, neck, lips, conjunctivae or hands, cutaneous candidiasis, hyperpigmentation, erythema nodosum. Allergic reactions ranging from urticaria to anaphylactic reactions have also been reported.
Renal/urogenital: interstitial nephritis, nephritis, renal failure, polyuria, urinary retention, urethral bleeding, vaginitis, acidosis, breast pain.
Musculoskeletal: arthralgia, or back pain, joint stiffness, achiness, neck or chest pain, flare up of gout.
Hemic/lymphatic: lymphadenopathy.
Special senses: blurred vision, disturbed vision (change in color perception, overbrightness of lights), decreased visual acuity, diplopia, eye pain, tinnitus, hearing loss, bad taste.
Adverse Laboratory Changes: Changes in laboratory parameters listed as adverse events without regard to drug relationship are as follows:
Hepatic: elevations of ALT (1.9%), AST (1.7%), alkaline phosphatase (0.8%), LDH (0.4%), serum bilirubin (0.3%).
Hematologic: eosinophilia (0.6%), leucopenia (0.4%), decreased blood platelets (0.1%), elevated blood platelets (0.1%), pancytopenia (0.1%).
Renal: elevations of serum creatinine (1.1%), BUN (0.9%), crystalluria, cylinduria, and hematuria have been reported.
Other changes reported in less than 0.1% of patients were: elevation of serum gammaglutamyl transferase, elevation of serum amylase, reduction in blood glucose, elevated uric acid, decrease in hemoglobin, anemia, bleeding diathesis, increase in blood monocytes, and leukocytosis.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image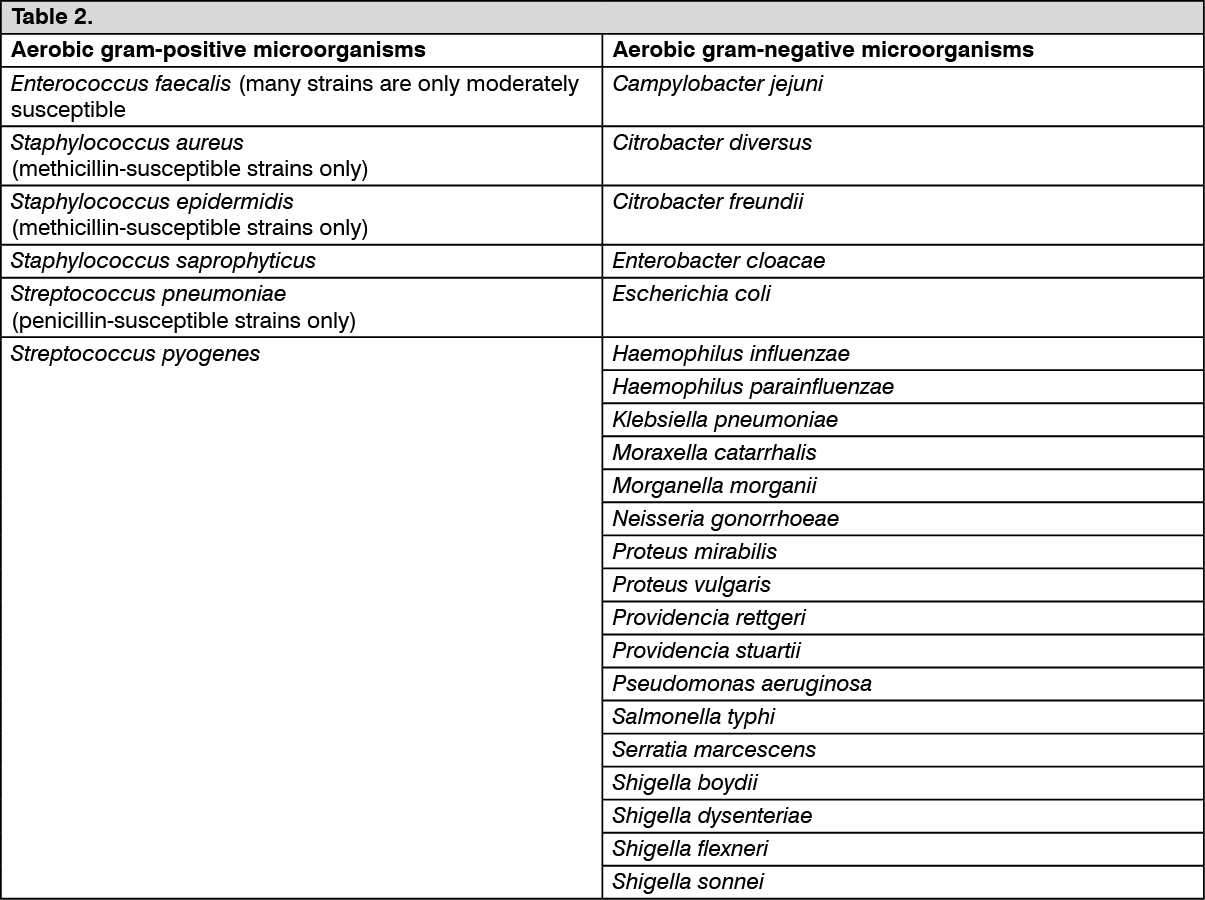 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image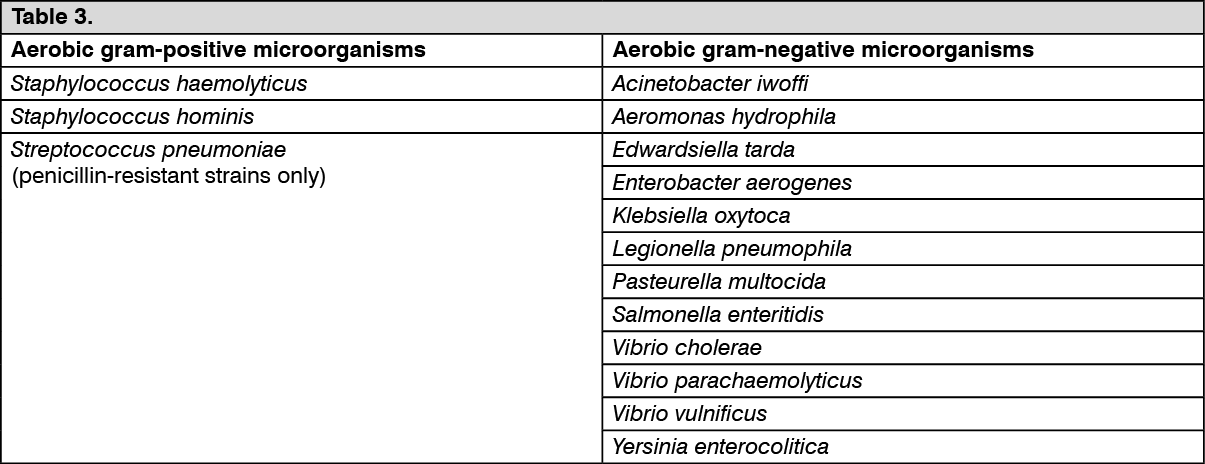 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image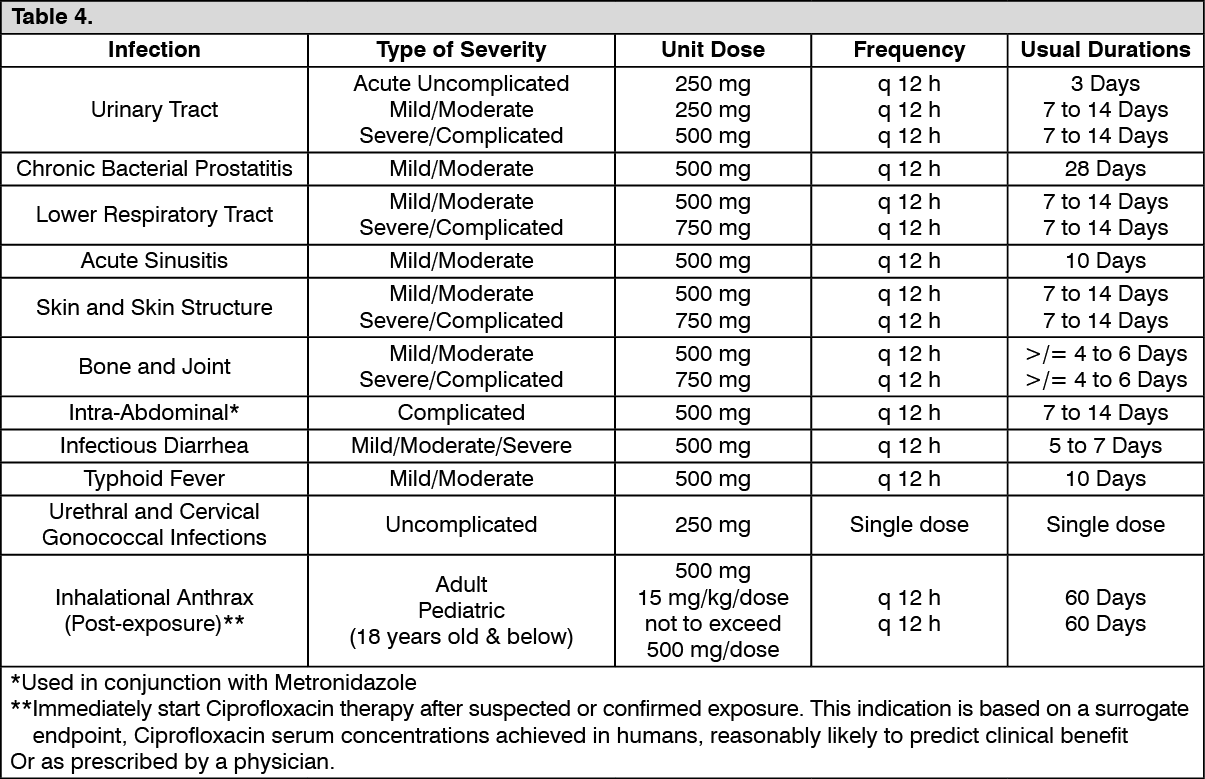 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out